
Cranial Neuropathies After Traumatic Brain Injury
Jun 22, 2026
Cranial neuropathies, caused by damage to the 12 cranial nerves, are a rare but serious consequence of traumatic brain injuries (TBI). These injuries often result in sensory or motor impairments like vision loss, facial paralysis, or difficulty swallowing, depending on the nerve affected.
Key points to know:
- Cranial Nerves I & II (Olfactory and Optic) are part of the central nervous system and are more prone to shearing injuries.
- Cranial Nerves III–XII originate from the brainstem and are more likely to recover due to the presence of Schwann cells.
- Traffic accidents are the leading cause of cranial nerve injuries, affecting younger individuals (average age: 44.3 years).
- Symptoms often include anosmia, diplopia, or nerve palsy, with delayed diagnosis being common.
Diagnosis involves neurological exams, CT or MRI imaging, and sometimes neurophysiological tests. Treatments range from observation and medications to surgical interventions like nerve decompression. Early detection and targeted care improve outcomes but require thorough evaluation and follow-up.
Ep 111 - Window to the Brain; Cranial Nerves, Brain Function & TBI Diagnosis w/ Dr. Uzma Samadani
Mechanisms and Epidemiology of Cranial Nerve Injury
Cranial Nerve Injuries After TBI: Key Statistics & Outcomes
Prevalence and Demographics
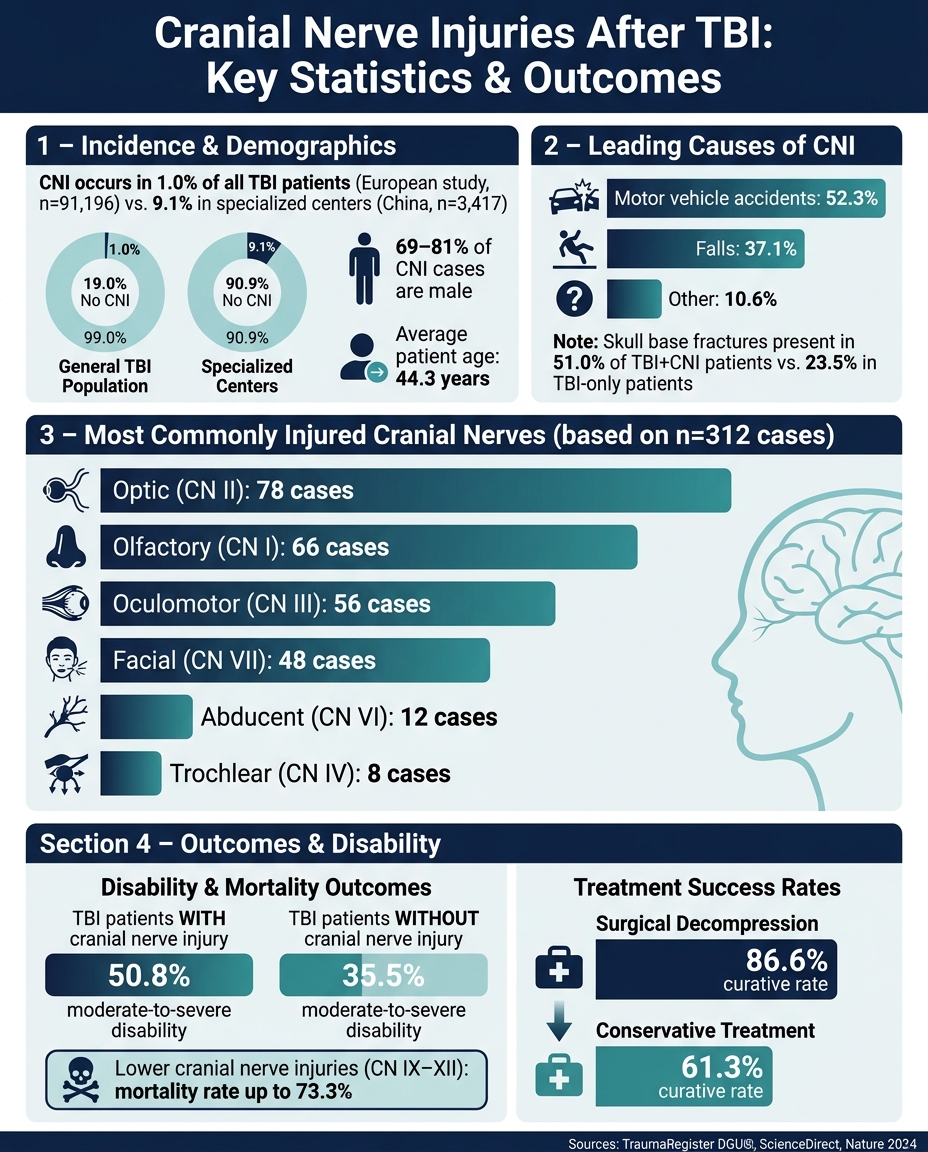
Cranial nerve injuries (CNI) following traumatic brain injury (TBI) are relatively rare but can have serious outcomes. A large European study of 91,196 TBI patients reported a CNI incidence of 1.0%. In contrast, data from a specialized treatment center in China showed a significantly higher rate of 9.1% (312 out of 3,417 patients), highlighting how incidence rates can vary depending on clinical settings and the thoroughness of patient evaluation. These numbers provide critical context for understanding how cranial nerves are impacted by trauma. To better visualize these structures, you can learn human anatomy through detailed courses and labs.
Men account for 69% to 81% of CNI cases, and affected individuals tend to be younger compared to the broader TBI population. This age distribution aligns with the fact that motor vehicle accidents, which are more common among younger people, are the leading cause of CNI, contributing to 52.3% of cases, while falls account for 37.1%.
How Cranial Nerves Get Injured
Cranial nerve damage in TBI often results from compression by bone fragments caused by skull base fractures, especially where nerves pass through narrow foraminal openings in the skull. As Professor Lijun Hou explains:
"The mechanism of traumatic cranial nerve injury is related to compression of the cranial nerves by bone fragments from fracture of the natural foramen of the skull base."
Other mechanisms include nerve traction, vascular compromise, or intraneural hemorrhage. Skull base fractures are a key factor, occurring in 51.0% of TBI patients with CNI, compared to just 23.5% in TBI patients without nerve injuries.
The type of skull fracture often determines the pattern of nerve damage. Lateral skull base fractures are closely associated with facial nerve palsy and hearing loss, while occipital condyle fractures are linked to dysfunction of the lower cranial nerves (IX–XII). Among survivors of occipital condyle fractures, cranial nerve dysfunction is relatively common, and multiple lower cranial nerves are often involved. These patterns reflect the varying susceptibility of specific cranial nerves to different trauma mechanisms.
Which Cranial Nerves Are Most Often Affected
Certain cranial nerves are more vulnerable to injury due to their anatomical positioning and the mechanisms of trauma. In a study of 312 CNI cases, the optic nerve (II) was the most frequently injured, followed by the olfactory (I) and oculomotor (III) nerves. The table below outlines the distribution of injuries and the primary vulnerabilities for each nerve:
| Cranial Nerve | Cases (n=312) | Primary Vulnerability |
|---|---|---|
| Optic (II) | 78 | Force transfer to optic canal; shearing at sclera |
| Olfactory (I) | 66 | Shearing of rootlets at cribriform plate |
| Oculomotor (III) | 56 | Brainstem displacement; hematoma compression |
| Facial (VII) | 48 | Temporal bone/lateral skull base fractures |
| Abducent (VI) | 12 | Long intracranial course; skull base fracture |
| Trochlear (IV) | 8 | Longest/smallest nerve; tentorial edge compression |
The trochlear nerve (IV), being the smallest and having the longest intracranial course, is particularly susceptible to compression against the tentorial edge during contrecoup injuries. On the other hand, injuries to the lower cranial nerves (IX–XII), though less common, are far more severe. These injuries are associated with mortality rates as high as 73.3%, reflecting their close association with severe trauma to regions controlling vital functions.
Neuroanatomy and Clinical Symptoms
Key Anatomical Structures
Understanding the vulnerable cranial nerve landmarks is crucial to grasp how injuries occur after traumatic brain injury (TBI). Certain key anatomical structures are especially prone to damage in this context.
The cribriform plate - a thin, perforated bone at the roof of the nasal cavity - allows the passage of olfactory nerve rootlets from the nose to the brain. These unmyelinated rootlets are highly vulnerable to shearing forces during head trauma. The optic canal, a narrow passage in the sphenoid bone, is another critical site where the optic nerve can be injured. Additionally, the nerve is at risk along its intracranial path near the falciform ligament. For the oculomotor nerve, the posterior petroclinoid ligament becomes a potential compression point when brainstem displacement occurs during trauma.
The jugular foramen, located at the base of the skull, serves as the exit point for cranial nerves IX, X, and XI. While injuries here are rare, they are extremely dangerous when they do occur.
These anatomical vulnerabilities directly influence the clinical symptoms seen in patients with TBI.
Symptoms by Cranial Nerve
The table below links specific cranial nerves, their anatomical sites, and the symptoms commonly observed after TBI:
| Cranial Nerve | Key Anatomical Site | Common Symptoms After TBI |
|---|---|---|
| I (Olfactory) | Cribriform plate | Anosmia, dysosmia |
| II (Optic) | Optic canal | Vision loss, afferent pupillary defect (APD) |
| III (Oculomotor) | Posterior petroclinoid ligament | Ptosis, dilated pupil, ophthalmoplegia |
| IV (Trochlear) | Free tentorial edge | Vertical or oblique diplopia |
| V (Trigeminal) | Petrous apex, facial foramina | Facial numbness, neuropathic pain, masticator weakness |
| VI (Abducens) | Dorello's canal | Horizontal diplopia (abduction defect) |
| VII (Facial) | Fallopian canal (temporal bone) | Facial paralysis, loss of taste (anterior two-thirds of tongue) |
| VIII (Vestibulocochlear) | Internal auditory canal | Hearing loss, vertigo, tinnitus |
| IX, X, XI | Jugular foramen | Dysphagia, hoarseness, shoulder weakness |
| XII (Hypoglossal) | Hypoglossal canal | Tongue deviation and atrophy |
Olfactory deficits, such as anosmia, are frequently overlooked and may be under‑reported by patients, underscoring the importance of specific testing. This highlights the importance of specific testing for such deficits. Similarly, optic nerve injuries - occurring in a minority of head injuries but representing a serious complication when present - can be detected early using a swinging flashlight test. This test identifies a relative afferent pupillary defect (APD), which can precede noticeable vision loss.
When injuries involve multiple regions, overlapping symptoms often arise.
When Multiple Cranial Nerves Are Injured
Injuries affecting multiple cranial nerves often indicate high-energy trauma and are associated with lower Glasgow Coma Scale (GCS) scores, severe fractures, and worse outcomes.
The anatomical layout of certain regions explains why these multi-nerve injury patterns occur. For instance, the cavernous sinus, a venous structure at the skull base, houses cranial nerves III, IV, V1, V2, and VI in close proximity. A single traumatic event or a post-traumatic carotid-cavernous fistula can damage all of these nerves simultaneously. Similarly, the orbital apex is a dense cluster of nerves, including II, III, IV, V1, and VI, making it another hotspot for multi-nerve injuries. Common combinations include CN III and VI, CN V and VI, and CN V and VII.
"Concomitant cranial nerve lesions indicate poorer functional outcome in traumatic brain injury patients." - Clinical Neurology and Neurosurgery
Some deficits, such as olfactory and optic dysfunction, may not become evident until days or weeks after the injury. This delay can result from progressive edema, fibrous tissue formation, or secondary vascular issues. These delayed symptoms emphasize the need for thorough and repeated neurological evaluations in TBI patients.
Diagnosing Cranial Neuropathies
Clinical Examination and Initial Assessment
Diagnosing cranial nerve injuries begins with a detailed neurological exam. However, if the patient has an altered level of consciousness, completing this assessment might need to wait until their mental status improves. Once feasible, a full cranial nerve evaluation should be conducted and repeated at key intervals. For example, in cases of occipital condyle fractures, serial cranial nerve testing at admission and during the first days of hospitalization, with reassessment before discharge, is recommended because some deficits may appear later. This repetition is crucial because some deficits may not be evident during the initial examination. Additionally, any detected cranial nerve deficit should raise concerns about the possibility of an underlying skull base fracture.
"Cranial nerve injuries... indicate a higher likelihood of functional impairment following primary care and complicating skull base fractures should be suspected." - TraumaRegister DGU®
Once the clinical evaluation is complete, imaging studies play a key role in identifying the structural cause of the injury.
Imaging Techniques
Imaging confirms the structural basis of cranial nerve deficits. CT scans are often the first choice in acute settings due to their speed and availability. They are particularly effective at identifying skull base fractures, bone fragments, and foraminal narrowing that may compress nerves.
For a more detailed view, MRI is generally the preferred modality for assessing the nerves themselves. It offers superior soft-tissue contrast, making it possible to detect subtle changes like nerve thickening, edema, or enhancement that might go unnoticed on CT. For instance, a study at NIMHANS hospital reported that in six patients with isolated oculomotor nerve palsy after mild TBI, CT scans showed no abnormalities, but high-resolution contrast-enhanced MRI revealed cisternal nerve thickening and enhancement. This guided targeted steroid therapy, leading to partial recovery.
To maximize clarity, cranial nerves I through VI are best viewed in the coronal plane, while nerves VII through XII are better seen in the axial plane. Using gadolinium contrast is frequently helpful, because nerve enhancement can be a key sign of injury that may not be apparent on non‑contrast imaging.
| Imaging Modality | Best Used For | Key Limitation |
|---|---|---|
| CT | Acute fractures, bone fragments, foraminal narrowing | Limited soft-tissue detail; may miss nerve-level issues |
| Standard MRI | Nerve parenchyma, edema, major structural changes | Subtle enhancements may go undetected without contrast |
| CE-MRI (with gadolinium) | Nerve enhancement, neuritis, small lesions | Requires patient stability; slower than CT |
| High-resolution 3D sequences (CISS/FIESTA) | Cisternal nerve segments (CN III–XII) | Susceptibility artifacts near bone and air |
| 3D Black Blood MRI | Subtle nerve enhancement near vessels | Limited availability |
If imaging results are inconclusive or the patient cannot cooperate, neurophysiological tests can provide additional insights.
Neurophysiological Testing
When clinical exams or imaging fail to provide clear answers, or if the patient cannot actively participate, neurophysiological testing becomes an important tool. These tests help differentiate true cranial neuropathies from conditions like myasthenia gravis.
For the facial nerve (CN VII), electromyography (EMG) and nerve conduction studies (NCS) serve as the primary diagnostic methods. Needle EMG should assess at least four of the five terminal branches for a comprehensive evaluation of dysfunction. For the vestibulocochlear nerve (CN VIII), the Auditory Brainstem Response (ABR) test is especially useful for assessing nerve and brainstem integrity in patients unable to complete standard audiometry.
"Auditory brainstem response has value for assessing brainstem and CN integrity in patients unable to participate in an audiogram." - Neupsy Key
Other tools, like the blink reflex test, allow for simultaneous evaluation of the trigeminal nerve (CN V) and the facial nerve (CN VII). For assessing the olfactory nerve (CN I), chemosensory evoked response potentials (CSERPs) provide an objective measure of olfactory function.
Treatment and Rehabilitation
Medical Treatments
Recent findings suggest exercising caution when using medications for cranial neuropathies. A 2024 systematic review published in Nature found no clear benefit from commonly used treatments for traumatic optic neuropathy (TON), such as intravenous methylprednisolone (IVMP), erythropoietin (EPO), or levodopa-carbidopa. Despite this, systemic corticosteroids are still used in 64% of trauma centers to address TON. However, high-dose corticosteroids - often referred to as "megadoses" - carry serious risks. The CRASH study, which tracked 10,008 patients with traumatic brain injuries (TBI), revealed that such treatments increased the likelihood of death or severe disability.
"There is no evidence of benefit for any pharmacologic or surgical intervention in treatment of TON [Traumatic Optic Neuropathy]. There is strong evidence of harm for treatment with megadose corticosteroids." - Nature, 2024
For orbital compartment syndrome, immediate treatment to reduce pressure is advised. This involves urgent measures to lower intraocular pressure and decompress the orbit, using medical and surgical interventions. In cases of isolated oculomotor nerve palsy following mild TBI, targeted steroid therapy has shown some potential for partial recovery.
Surgical Interventions
When medications fail or imaging reveals direct nerve compression, surgical options come into play. For TON, transnasal endoscopic optic nerve decompression has shown a clinical success rate of 69.2%. Notably, patients with residual light perception before surgery experience an 85.7% success rate for visual improvement, compared to a 50% success rate in those without light perception.
"Transnasal endoscopic optic nerve decompression is an effective treatment method for TON. The presence of residual light perception and the timing of surgery within 7 days are crucial to the prognosis." - Xiang Tu, et al.
In cases of facial nerve injuries related to temporal bone fractures, electroneuronography (ENoG) plays a key role in surgical decision-making. A loss of more than 90% in action potential amplitude is often the threshold for considering decompression surgery. Complete paralysis that occurs immediately usually points to nerve transection, which often requires surgery. In contrast, delayed-onset palsy is more likely caused by edema or ischemia, making medical management the initial approach.
For infraorbital nerve injuries caused by zygomaticomaxillary complex fractures, surgical decompression appears to have better sensory recovery when performed early after injury, such as within the first few weeks.
"Surgical decompression performed early after injury significantly improves sensory recovery outcomes over conservative management." - Unnati Bimal Mehta, et al.
Rehabilitation Strategies
Once acute treatments are addressed, structured rehabilitation becomes a critical step in recovery. For trochlear nerve (CN IV) injuries causing diplopia, initial management often involves eye patches and prisms. If no progress is seen after a year of conservative treatment, eye muscle surgery may be considered.
In oculomotor nerve (CN III) palsy, non-surgical options like guided eye movement rehabilitation and botulinum toxin injections can help manage muscle imbalances, though full recovery is rare.
Olfactory dysfunction is usually managed conservatively, as the olfactory pathway has a natural ability to regenerate. For trigeminal nerve involvement, it’s recommended to monitor the patient with serial neurological evaluations for up to three months before deciding on surgical exploration. Additionally, in cases of indirect optic nerve injuries, conservative observation alone can lead to substantial spontaneous visual recovery in a significant proportion of patients, highlighting the value of watchful waiting combined with regular follow-up care.
Future Directions in Research
Emerging studies are continuously shifting how we understand post-traumatic cranial neuropathies, offering new perspectives on diagnosis and management.
Advances in Imaging and Biomarkers
Traditional imaging methods like CT and MRI often fail to detect subtle cranial nerve injuries, particularly in cases of mild TBI. However, advanced imaging techniques are stepping in to fill these gaps, providing a more detailed look at microstructural nerve changes.
One such technique is Diffusion Basis Spectrum Imaging (DBSI). Unlike the more commonly used Diffusion Tensor Imaging (DTI), which struggles with overlapping signals from injuries, DBSI can separately measure axonal loss, myelin damage, and inflammation. Preclinical studies have shown a strong correlation between DBSI-derived axon volume and histological evidence of axonal loss (r² = 0.4918, p = 0.0002). These findings suggest DBSI has potential for identifying subclinical traumatic optic neuropathy, although current evidence is largely from animal and early human studies.
Another promising tool is Ultra-High Contrast (UHC) MRI, which employs dSIR sequences to detect white matter changes that standard scans miss. A study conducted in December 2025 identified the "whiteout sign" on dSIR images in 25 of 29 TBI patients, compared to just 3 of 37 healthy controls. This finding was linked to a significantly higher odds ratio (14 or more) for symptomatic TBI status. Inter-reader reliability for detecting the whiteout sign was notably high (κ = 0.85). Daniel Cornfeld from Matai Medical Research Institute emphasized its potential:
"The whiteout sign was strongly associated with being in the symptomatic group and is a potential biomarker for recognition of secondary changes to the brain in patients with persistent symptoms following TBI."
Other advanced MRI techniques, including sequences that suppress vascular signal and MR neurography, are being developed to improve visualization of small cranial nerves, although evidence in TBI-related cranial neuropathies remains limited. Researchers are also exploring network-wide analyses using tools like the Structural Network Fingerprint (SNF) to identify injury patterns across systems like the Default Mode Network.
These advancements are paving the way for earlier diagnoses and more precise treatments for cranial neuropathies.
Long-Term Outcomes and Multidisciplinary Collaboration
While imaging breakthroughs are crucial, long-term patient outcomes hinge on comprehensive care plans. Data shows that TBI patients with cranial nerve injuries have higher rates of moderate to severe disability than TBI patients without cranial nerve involvement, suggesting that such injuries may be under-recognized.
Longitudinal research highlights that recovery is influenced not only by the specific nerve affected but also by the mechanism of injury. For instance, in cases of trigeminal neuropathy, "positive" sensory symptoms like allodynia and hyperesthesia tend to have a greater negative impact on quality of life than simple sensory loss. Predictive models based on initial assessments have shown a negative predictive value of 87% for sensory recovery in trigeminal neuropathy after six months, helping clinicians set realistic recovery expectations.
Improving outcomes will require closer collaboration between specialists. Neuroprotective treatments often need to be administered within hours of an injury, demanding seamless coordination among trauma experts, neurologists, and radiologists. As noted in Nature/Eye:
"To improve the opportunities for research in this area, the first step will be to improve the likelihood of diagnosis in affected patients, which would require closer working with trauma specialists and may also drive greater consideration of systemic safety data."
The emerging field of oculomics, which examines the eye as a diagnostic tool for broader brain health, may help detect subtle retinal and optic nerve changes linked to broader brain health, although its role in traumatic optic nerve injury is still being explored.
Conclusion
Cranial neuropathies following traumatic brain injuries (TBI) are more common and impactful than often recognized. They occur in about 1.0% of all TBI cases and rise to 9.1% in specialized treatment centers. The consequences are significant, with patients who have cranial nerve involvement showing higher rates of moderate to severe disability than TBI patients without nerve involvement.
Early detection plays a key role in managing these injuries. Subtle signs, like anisocoria or an afferent pupillary defect, can point to nerve damage that may not appear on standard imaging. Importantly, contemporary evidence does not support megadose corticosteroids as a beneficial treatment for traumatic optic neuropathy, and concerns have been raised about potential harm. In contrast, surgical decompression, when appropriate, has been associated with higher recovery rates in some series (for example, 86.6% vs 61.3% with conservative treatment in one study). A thorough understanding of anatomy is essential to determine when and how to intervene.
Understanding the intricate relationship between trauma mechanisms and nerve pathways is crucial for effective treatment. Resources like the Institute of Human Anatomy, which utilize real cadavers to teach anatomy, provide valuable insights. For instance, knowing how the olfactory nerve passes through the cribriform plate or where the oculomotor nerve exits the dura helps clinicians interpret symptoms, select imaging tools, and prioritize interventions.
"It is necessary to standardize surgical indications, operation timing, surgical approaches and methods for the treatment of TBI-complicated cranial nerve injury." - ScienceDirect
Improving outcomes for TBI patients will depend on better diagnostics, stronger multidisciplinary collaboration, and a deeper understanding of anatomy. These elements together can pave the way for more effective interventions and recovery.
FAQs
What TBI symptoms suggest a cranial nerve injury?
Cranial nerve injuries following a traumatic brain injury (TBI) often lead to distinct sensory or motor issues. Some key indicators include anisocoria (unequal pupil size) and oculomotor nerve palsies, such as third cranial nerve palsy, which can manifest as fixed, dilated pupils. Depending on which nerve is affected, symptoms may range from problems with smell or balance to facial nerve dysfunction. Identifying these signs is crucial for accurate diagnosis and treatment.
What tests confirm a cranial neuropathy after head trauma?
Diagnosing cranial neuropathy after head trauma requires a detailed neurologic examination and specific diagnostic tests. These assessments focus on key functions like vision, pupillary responses, facial muscle movement, and hearing to identify any abnormalities.
Imaging plays a central role in the process. CT scans are used to identify fractures, while high-resolution MRI is better suited for detecting issues with nerves or blood vessels. In some cases, electromyography (EMG) and nerve conduction studies are employed to assess the condition of the affected nerves.
Given the complexity of head trauma cases, repeat evaluations are often necessary to monitor changes in the patient's condition over time.
When is surgery needed instead of watchful waiting?
Surgery is typically advised for cranial neuropathies in certain situations, such as nerve transections (like facial nerve injuries) or traumatic nerve compression caused by fractures, including those in the superior orbital fissure. When it comes to ocular motor nerve palsies, surgical intervention is generally considered only after a period of observation to allow for spontaneous recovery, with timing individualized based on clinical course and specialist assessment. In most other cases, non-surgical approaches - such as steroids or rehabilitation - are usually the first line of treatment.

