
Thyroid Function and Aging: What Changes
Apr 15, 2026
As we age, thyroid function naturally shifts, leading to changes in hormone levels and how the body responds to them. Here's the key takeaway:
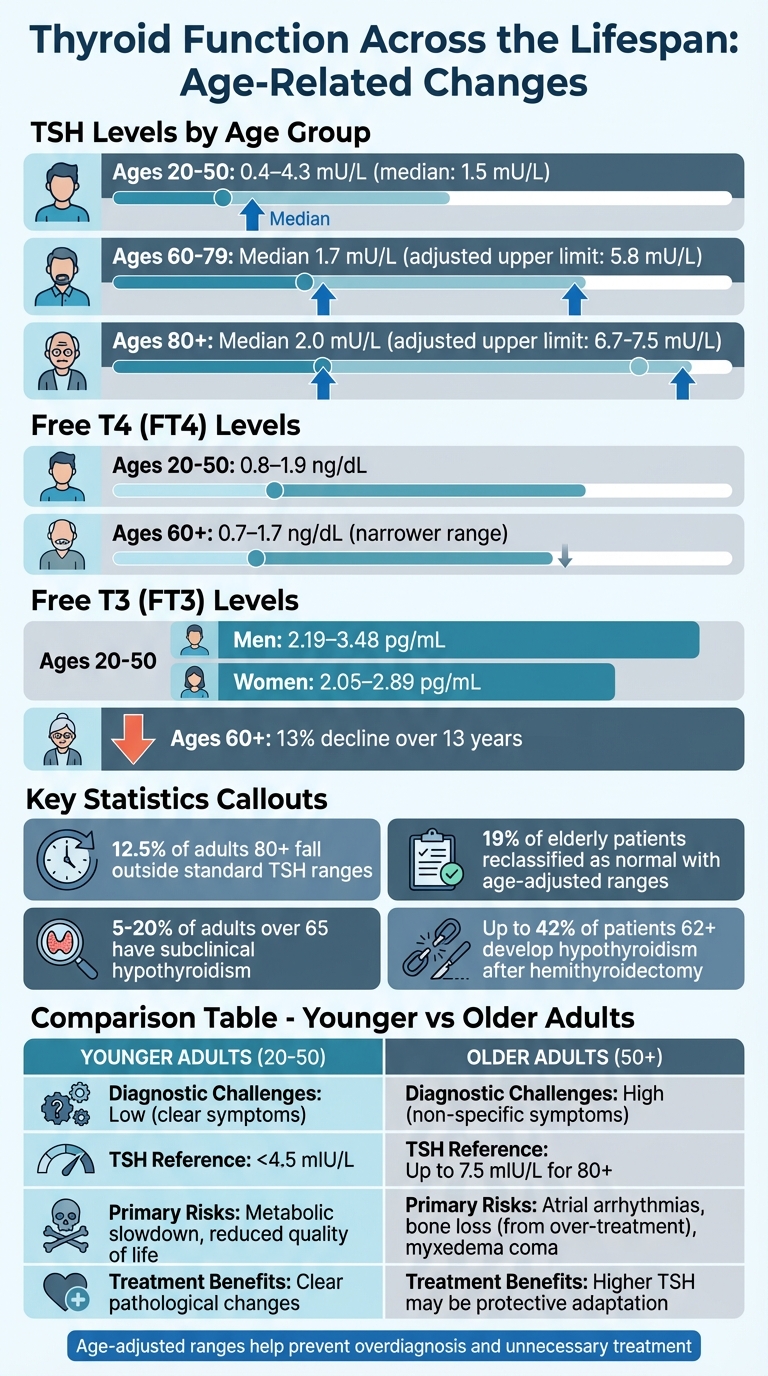
- TSH Levels Increase with Age: By age 80, TSH levels can rise to 6.7 mIU/L or higher, often without signaling illness.
- T3 levels decline with age: While free T4 tends to remain stable or change only slightly; overall, thyroid hormone levels in healthy older adults usually stay within age‑appropriate reference ranges.
- Subclinical Hypothyroidism is Common: 5-20% of adults over 65 have elevated TSH with normal T3/T4 levels, often without symptoms.
- Symptoms Overlap with Aging: Fatigue, weakness, and shortness of breath make diagnosis tricky in older adults.
- Treatment Risks: Over-treating with thyroid hormones can cause heart rhythm issues and bone loss in older adults.
Age-specific TSH ranges and careful evaluation are essential to avoid misdiagnosis or unnecessary treatments. Let’s dive into how thyroid function evolves across different age groups and why it matters.
Thyroid Function Changes by Age: TSH, T3, and T4 Reference Ranges
Sex, Fat, & Weight Loss | The Gland That Controls It All
1. Adults Ages 20-50
For adults between 20 and 50 years old, thyroid function tends to remain steady, showing a predictable pattern distinct from the changes that occur later in life.
TSH Levels
TSH levels in this age group are typically stable, falling within a reference range of 0.4–4.3 mU/L, with a median value of about 1.5 mU/L. Interestingly, women tend to have slightly higher TSH levels than men, which can complicate diagnoses. For example, in some cohorts, applying age‑ and sex‑specific TSH intervals reclassifies a large proportion of women previously labelled abnormal as normal, whereas the impact is smaller in middle‑aged men. Alongside TSH, thyroid hormone levels also follow clear patterns in this age range.
FT3 and FT4 Levels
Free T4 (FT4) levels for younger adults range from 0.8 to 1.9 ng/dL, with men generally showing slightly higher levels than women. Free T3 (FT3) levels also vary by gender: men typically have levels between 2.19 and 3.48 pg/mL, while women range from 2.05 to 2.89 pg/mL.
Hypothalamic-Pituitary-Thyroid Axis Response
The stability of these hormone levels is guided by the hypothalamic-pituitary-thyroid axis, which maintains a precise inverse log-linear relationship between TSH and FT4 levels. This makes TSH the most sensitive marker for thyroid screening in this age group.
Health Outcomes
In younger adults, even mild TSH elevations may indicate early thyroid dysfunction and have been associated in some studies with dyslipidemia, adverse cardiovascular outcomes, and pregnancy complications, particularly when TSH is ≥10 mIU/L. Associations for smaller TSH rises are weaker and less consistent. Additionally, factors such as pregnancy, smoking, recent hospitalizations, and certain medications (like amiodarone, corticosteroids, lithium, and dopamine agonists) can influence thyroid function tests.
2. Adults Ages 50 and Older
Thyroid function tends to shift noticeably after age 50, unlike the more stable patterns seen in younger adults. These changes are usually part of the body's normal adaptation to aging rather than signs of illness. However, they can complicate diagnosis and treatment choices.
TSH Levels
As people age, TSH levels gradually increase. For example, the median TSH level rises from about 1.5 mU/L in younger adults to 1.7 mU/L in those aged 60–79, and 2.0 mU/L for individuals 80 and older. Standard lab ranges (0.4–4.5 mU/L) often misclassify older adults as hypothyroid. Specifically, 6.5% of adults aged 60–79 and 12.5% of those 80 and older fall outside these ranges. Adjusting the upper limit of TSH to 5.8 mU/L for ages 60–79 and 6.7 mU/L for those 80 and above can reclassify around 19% of elderly patients as having normal thyroid function. These shifts align with natural declines in thyroid hormone levels.
FT3 and FT4 Levels
In older adults, FT3 clearly declines with age, whereas FT4 tends to remain relatively stable, with small increases or decreases depending on the population. Many labs use slightly narrower FT4 ranges for adults over 60. Total T3 levels also drop - by about 13% over 13 years in older adults. This decline may actually serve a protective role by reducing catabolism. Interestingly, findings from the Leiden 85+ Study revealed that participants with higher TSH levels tended to have better survival, suggesting that mildly higher TSH may be benign or even advantageous in very old age.
Hypothalamic-Pituitary-Thyroid Axis Response
The aging process impacts the thyroid's regulatory axis, reducing its sensitivity to feedback and altering hormone metabolism. Age-related changes, such as thyroid atrophy, fibrosis, and decreased 5'-deiodinase activity, lead to a weaker TSH response and lower T3 production.
Health Outcomes
Understanding these age-related thyroid changes is crucial for avoiding overtreatment and tailoring care more effectively. For instance, In older adults, isolated TSH elevation with normal FT4 (especially when TSH is <7–10 mIU/L) usually does not require treatment, unless there are clear symptoms or other risk factors. Over-replacement of thyroid hormones can increase the risk of complications like atrial fibrillation and osteoporotic fractures. On the other hand, untreated hypothyroidism can lead to serious issues, including myxedema coma and complications during surgery. Additionally, hypothyroidism is common after hemithyroidectomy and radioactive iodine in older adults: studies report that roughly one‑third to over 40% of older patients may become hypothyroid after hemithyroidectomy, and about 20–60% develop hypothyroidism within several years after radioiodine, depending on dose and indication.
Pros and Cons of Age-Related Thyroid Changes
As we age, thyroid function naturally shifts, bringing both protective benefits and potential challenges in diagnosis and treatment.
For instance, the rise in TSH (thyroid-stimulating hormone) levels commonly seen in older adults might actually serve a protective role. Research from the Leiden 85+ Study revealed that participants with elevated TSH levels experienced better overall survival rates. Similarly, a gradual 13% reduction in total T3 levels over 13 years among healthy elderly individuals may help reduce catabolism. However, these same changes complicate diagnosis. For example, about 12% of individuals aged 80 and older have TSH levels exceeding 4.5 mIU/L without any signs of autoimmune thyroiditis, making it harder to pinpoint thyroid disorders.
Treatment poses its own risks, especially when it comes to overtreatment. Overprescribing levothyroxine in elderly patients can lead to serious issues like atrial arrhythmias and increased bone loss.
"Specific attention should be paid to minimizing the risks of atrial arrhythmias and progressive bone loss that may be associated with iatrogenic thyrotoxicosis caused by over-treatment".
On the other hand, failing to treat hypothyroidism can raise surgical risks, including complications during and after operations.
Here’s a comparison of how thyroid changes differ between younger and older adults:
| Feature | Younger Adults (20-50) | Older Adults (50+) |
|---|---|---|
| Primary Health Risks | Standard metabolic slowdown; reduced quality of life | Atrial arrhythmias, bone loss (from over-treatment), myxedema coma, and increased mortality |
| Diagnostic Challenges | Generally low; symptoms are clear and "classic" | High; symptoms are non-specific and confounded by other diseases |
| TSH Reference Ranges | Standard ranges (typically < 4.5 mIU/L) are usually appropriate | Age-adjusted ranges (up to 7.5 mIU/L for age 80+) prevent over-treatment |
| Potential Benefits of Changes | N/A (Changes are typically pathological) | Higher TSH may be a physiological adaptation; lower T3 may be a marker of longevity |
| Surgical Risks | Standard operative risk | Higher risk of intraoperative hypotension, hyponatremia, and prolonged intubation |
Adjusting TSH reference ranges for older adults (up to 7.5 mIU/L for those over 80) helps reduce the likelihood of overtreatment and its associated complications, such as cardiac and skeletal issues. These functional changes also pave the way for structural changes in the thyroid as we age.
Goiter! Huge Thyroid Growth in Someone’s Neck!
Anatomical Changes in the Thyroid Gland with Age
As we age, the thyroid gland can undergo some structural changes, such as reduced volume and increased fibrosis, which may contribute to alterations in thyroid function. However, many age-related changes in thyroid hormone levels are also influenced by central regulatory mechanisms and adaptive processes.
Animal studies suggest that aging can lead to smaller thyroid follicles and reduced colloid content, potentially affecting hormone storage; however, evidence for this process as a major factor in human thyroid aging remains limited.
Additionally, thyroid activity is at its peak early in life and diminishes as we age. This decline is evident in the lower weight-based levothyroxine needs of adults compared to newborns. These physical changes align with the functional shifts already discussed.
Studies of cadavers provide further insights into these age-related changes. Research, including work from the Institute of Human Anatomy, has documented glandular atrophy, where functional thyroid tissue is replaced by fat and connective tissue. While internal structural changes occur with age, there is limited evidence that the position of the thyroid gland shifts significantly downward solely due to aging. Increased interfollicular fibrosis occurs with age; lymphocytic infiltration may be seen but is more typical of autoimmune conditions than normal aging.
These anatomical changes have a direct impact on thyroid function. Older individuals tend to have higher TSH levels for a given free T4 concentration compared to younger people; this may reflect altered regulatory set points or bioactivity rather than solely decreased cellular responsiveness.
"The hypothalamic pituitary thyroid axis is altered with age and older individuals have been shown to exhibit a blunted TSH response to thyroid hormone deficiency." – Thyroid Research Journal
Conclusion
Younger adults tend to show classic signs of hypothyroidism, like cold intolerance and weight gain. In contrast, older adults often report more subtle issues, such as fatigue, weakness, or shortness of breath. Notably, TSH levels naturally increase with age, and for individuals over 80, the upper limit can reach 7.5 mIU/L, compared to the standard 4.5 mIU/L threshold. This shift highlights the risk of overdiagnosing subclinical hypothyroidism in older adults when applying a one-size-fits-all reference range.
Community studies reveal that 7% to 14% of elderly individuals have TSH levels exceeding standard ranges, despite many being euthyroid. Furthermore, treating mild subclinical hypothyroidism in older adults has not been shown to improve cognitive or functional outcomes. On the flip side, overtreatment carries its own dangers, including atrial arrhythmias and accelerated bone loss.
"There is a strong case for implementing age-related reference ranges for TSH in adults to prevent an inappropriate diagnosis of subclinical hypothyroidism in older people and to discourage unnecessary levothyroxine prescribing." – John P. Walsh, Department of Endocrinology & Diabetes, Sir Charles Gairdner Hospital
These findings emphasize the need for age-specific diagnostic strategies. Clinicians should consider age-adjusted TSH ranges and confirm subclinical hypothyroidism with repeat testing, as TSH levels can normalize on their own. Treatment should also reflect these age-related differences. For example, older adults typically require lower levothyroxine doses (1.6 to 2.0 µg/kg/day) compared to neonates, who need higher doses (10 to 15 µg/kg/day) due to faster metabolic clearance.
FAQs
What TSH level is considered normal for my age?
For older adults, what's considered a normal TSH level can be a bit higher compared to younger people. Generally, levels up to 4.0–4.5 mIU/L are often seen as normal for this age group, but these ranges can differ depending on individual circumstances. Some experts suggest using age-specific reference ranges, so it’s a good idea to talk to your healthcare provider for advice tailored to your needs.
When does subclinical hypothyroidism need treatment in older adults?
When treating subclinical hypothyroidism in older adults, it's important to evaluate if TSH levels consistently remain above 10 μU/mL. This is particularly crucial if symptoms are noticeable or certain risk factors are present. Elevated TSH levels, along with antithyroid antibodies, can increase the likelihood of the condition advancing to overt hypothyroidism. In these situations, regular monitoring and timely intervention play a key role.
What can cause a temporary change in TSH on lab tests?
Temporary fluctuations in TSH levels can happen due to factors like acute illness, stress, pregnancy, or specific medications. These can momentarily affect TSH results without pointing to a lasting thyroid problem. If your TSH levels seem off, your healthcare provider will likely take these influences into account before diagnosing or suggesting additional tests.

