
Macrophages in Tissue Repair and Healing
Jun 16, 2026
Macrophages are immune cells that play a key role in tissue repair by cleaning debris, fighting pathogens, and guiding the healing process. They adapt their behavior across four key phases of tissue repair: hemostasis, inflammation, proliferation, and remodeling. Their ability to shift between pro-inflammatory and pro-repair states ensures proper healing, but disruptions can lead to chronic wounds or fibrosis. Understanding their roles - whether tissue-resident or monocyte-derived - is critical for learning human anatomy and grasping how tissues regenerate and recover from injury. This article breaks down macrophage functions, their impact on specific organs, and how they contribute to both repair and scarring.
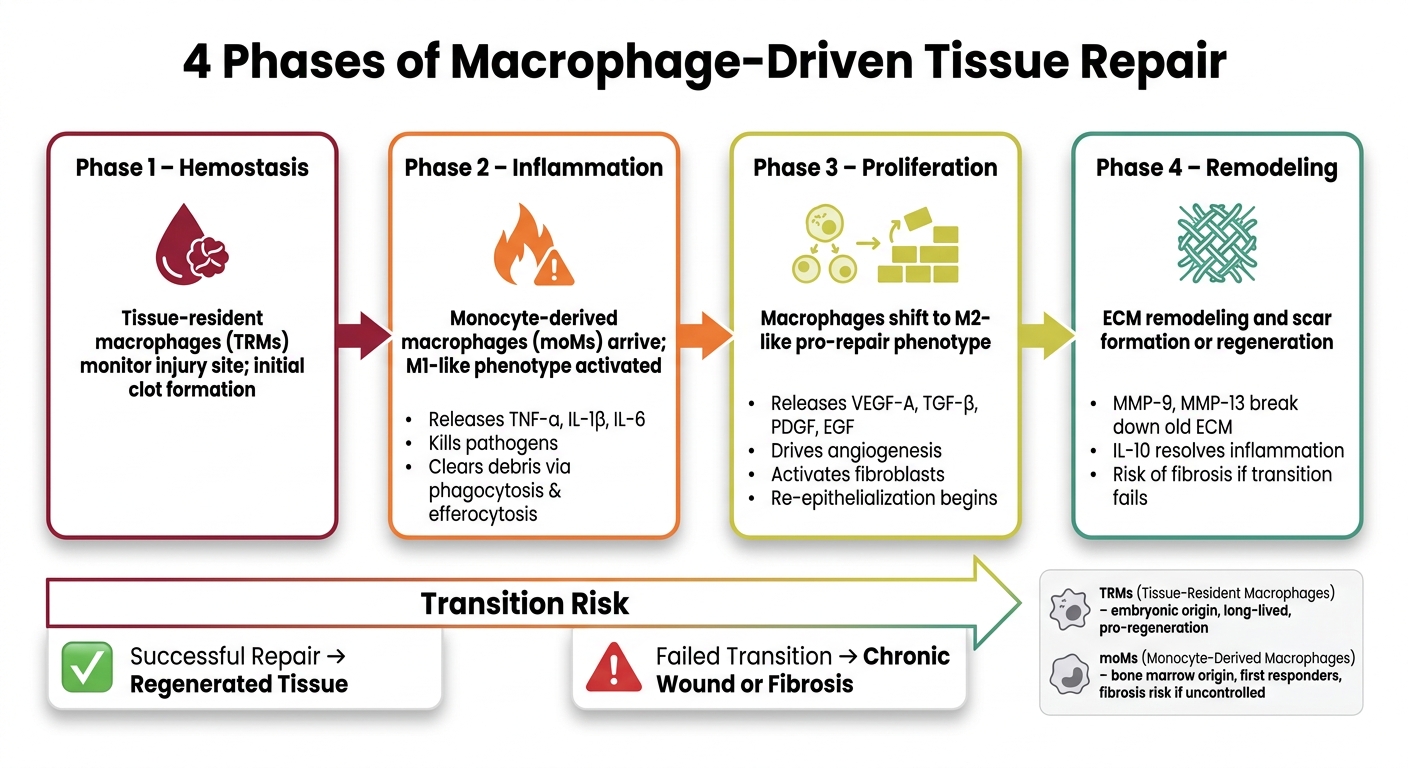
4 Phases of Macrophage-Driven Tissue Repair
Macrophage Types and Their Functions in Repair
Tissue-Resident vs. Monocyte-Derived Macrophages
The origin of macrophages plays a key role in determining how tissues heal after injury.
Tissue-resident macrophages (TRMs) come from embryonic precursors in the yolk sac or fetal liver and settle into tissues before birth. These cells are long-lived, self-renewing, and help maintain tissue health by constantly monitoring and managing local conditions.
Monocyte-derived macrophages (moMs), on the other hand, are formed in the bone marrow after birth. These cells circulate in the bloodstream and are quickly dispatched to injury sites. They act as first responders, managing acute inflammation and clearing debris, but they don’t stick around for the long haul.
"The developmental origin of injury-associated macrophages has a major impact on the outcome of the healing process." - Sebastian Willenborg, Department of Dermatology, University of Cologne
In simple terms, TRMs are often linked to tissue homeostasis and regenerative, low‑scarring outcomes, while moMs, though essential for immediate defense and repair, can contribute to fibrosis if their inflammatory and remodeling activities are not properly controlled. For instance, in the adult heart, injury is accompanied by an influx of CCR2⁺ inflammatory moMs that can partially replace embryo‑derived TRMs; when this response is excessive or prolonged, it is associated with more fibrotic remodeling and less regeneration. This highlights how the origin of macrophages influences their role in healing.
Proinflammatory and Pro-Repair Macrophage Phenotypes
When moMs arrive at an injury site, they predominantly adopt proinflammatory (M1‑like) phenotypes in the early phase. In this state, they release cytokines such as TNF-α, IL-1β, and IL-6 to fight off pathogens and clear debris. However, this inflammatory phase must eventually give way to repair processes to ensure proper healing.
As the situation stabilizes, macrophages shift toward more pro‑repair (M2‑like) phenotypes. In this state, they produce growth factors like TGF-β, VEGF, and PDGF, which support new blood vessel formation, tissue remodeling, and extracellular matrix (ECM) production.
| Feature | Proinflammatory (M1-like) | Pro-Repair (M2-like) |
|---|---|---|
| Key Stimuli | LPS, IFN-γ, TNF-α | IL-4, IL-13, IL-10 |
| Secreted Factors | TNF-α, IL-1β, IL-6, ROS | IL-10, TGF-β, VEGF, PDGF |
| Metabolism | Glycolysis | Fatty acid oxidation / OXPHOS |
| Main Role | Pathogen killing, debris clearance | Angiogenesis, ECM synthesis, remodeling |
One crucial mechanism driving this shift is efferocytosis, where macrophages engulf dying neutrophils. This process reduces the production of inflammatory cytokines and encourages tissue repair. When macrophages fail to make this transition, it can result in chronic wounds with ongoing inflammation.
Macrophage States as a Spectrum, Not a Binary
While the M1/M2 framework is helpful for understanding macrophage behavior, it oversimplifies their roles. Research increasingly shows that macrophages operate along a continuum of states, rather than fitting neatly into two categories.
"The M1/M2 concept is too simplistic, and in tissues macrophage function comprises a broad spectrum of activation phenotypes." - Sebastian Willenborg, Louise Injarabian, and Sabine A. Eming
For example, single-cell RNA sequencing has identified dozens of distinct macrophage subpopulations, each responding to unique combinations of signals. Many macrophages express markers from both M1 and M2 states at the same time, showing that their roles are more fluid than previously thought.
Additionally, macrophages are highly sensitive to mechanical cues, such as changes in tissue stiffness during healing. This adaptability, sometimes referred to as the "monocyte waterfall", reflects the gradual and overlapping transitions that monocytes undergo as they take on different functions.
Phagocytosis and Debris Clearance in Tissue Healing
How Phagocytosis Works
When tissue is damaged, debris and pathogens quickly pile up, and macrophages step in to clean up the mess before any repair can get underway.
Phagocytosis is the process where macrophages detect, engulf, and break down particles larger than 0.5 μm. This process happens in four stages: recognition, internalization, formation of a phagosome, and maturation into a phagolysosome packed with acid hydrolases. Macrophages are considered "professional" phagocytes because their lysosomal machinery is more specialized for high-capacity phagocytosis than that of fibroblasts or epithelial cells. But macrophages don't just engulf debris - they also release matrix metalloproteinases (MMPs) like MMP9 and MMP12. These enzymes break down the damaged extracellular matrix, clearing the way for new tissue to grow.
Efferocytosis and the Resolution of Inflammation
Macrophages take their cleanup role even further by initiating anti-inflammatory responses through a process called efferocytosis. This happens when macrophages remove apoptotic (dying) cells, but it's not just about tidying up.
Dying cells send out "find-me" signals, such as ATP, and display "eat-me" markers like phosphatidylserine, which attract macrophages. Specialized receptors on macrophages - such as MerTK, Axl, and Tim-4 - recognize these markers, often with help from bridging molecules like Gas6 and MFGE8. Meanwhile, healthy cells avoid being engulfed by showing "don't-eat-me signals" like CD47.
"Efferocytosis is no longer seen as a mere scavenging behavior but rather as a complex biological network that regulates local immune homeostasis, modulates the tissue microenvironment, and mediates regenerative processes." - Frontiers in Immunology
Once a macrophage engulfs an apoptotic cell, it undergoes a dramatic shift in function. This process suppresses pro-inflammatory pathways - like NF-κB and the NLRP3 inflammasome - while promoting the release of anti-inflammatory cytokines such as TGF-β and IL-10. In this way, efferocytosis not only reduces inflammation but also sends out signals to kickstart repair.
"Phagocytosis of apoptotic cells is important for the initiation of the mid-stage of wound healing because it represses the production of proinflammatory cytokines and stimulates the release of cell growth and proliferation factors by macrophages." - CSH Perspectives
What Studies Show About Phagocytosis Disruptions
Research has shown that when phagocytosis is disrupted, healing can stall or fail entirely. A 2024 study in Nature by Turan Tufan and Kodi S. Ravichandran from Washington University School of Medicine provides a striking example. The researchers used zebrafish embryos lacking the transcription factor EGR3 and observed that microglia - the brain's resident macrophages - struggled to clear apoptotic neurons. These cells showed fewer maturing phagosomes, directly linking EGR3 loss to defective debris processing in a living organism.
The issue stems from a mechanism called RNA polymerase II (Pol II) pause/release, which allows macrophages to quickly reprogram their genes when they encounter a dead cell. Without this system, macrophages can handle one apoptotic cell but struggle to process others, leading to a dangerous buildup of debris.
"Macrophages use Pol II pause/release as a mechanism to rapidly alter their transcriptional programs for efficient processing of the ingested apoptotic corpses and for successive efferocytosis." - Turan Tufan and Kodi S. Ravichandran, Division of Immunobiology, Washington University School of Medicine
In diabetic wounds, impaired efferocytosis leads to the accumulation of dead cells, which eventually undergo secondary necrosis. This releases pro-inflammatory substances that trap macrophages in an M1-like inflammatory state. This dysfunction is one of the key reasons why diabetic wounds are so challenging to heal, as it prevents the critical transition from inflammation to tissue repair - a topic explored further in the next section on tissue regeneration.
How Macrophages Drive Tissue Regeneration
Growth Factors and Cytokines Released During Healing
Once the inflammatory phase winds down, macrophages take on a new role: guiding tissue reconstruction. Think of them as foremen on a construction site, directing cells on what to build and where. They release a cocktail of growth factors that kickstart the repair process.
One standout signal is VEGF-A, which is crucial for angiogenesis - the formation of new blood vessels. This ensures that healing tissues get the oxygen and nutrients they need. During early and mid-stage wound healing, macrophages are a major source of VEGF in granulation tissue. Beyond VEGF-A, macrophages produce TGF-β and PDGF, which help activate fibroblasts and promote their differentiation into contractile myofibroblasts that close wounds and rebuild the extracellular matrix (ECM). Meanwhile, EGF helps keratinocytes grow and aids in re-epithelialization, while IGF-1 and Wnt proteins steer stem and progenitor cells to regenerate damaged tissue.
"Macrophages regulate tissue regeneration following injury... they produce a variety of growth factors, such as IGF-1, VEGF-α, TGF-β, and Wnt proteins that regulate epithelial and endothelial cell proliferation." - Kevin M. Vannella, National Institute of Allergy and Infectious Diseases
Here’s a quick overview of what these factors do:
| Factor | Primary Function |
|---|---|
| VEGF-A, FGF-2 | Promote angiogenesis (new blood vessel growth) |
| TGF-β, PDGF | Activate fibroblasts; drive ECM and collagen synthesis |
| EGF | Stimulate keratinocyte growth and wound closure |
| IGF-1, Wnt proteins | Guide stem cell differentiation and tissue regeneration |
| MMP-9, MMP-13 | Contribute to degradation of extracellular matrix components during remodeling |
| IL-10 | Reduce inflammation and shift to repair mode |
These factors aren’t one-size-fits-all. Their roles vary depending on the tissue and the specific context of the injury.
Macrophage Roles in Specific Organs
While growth factors initiate repair, macrophages adapt their behavior based on the tissue they’re working in. The local environment shapes how they function.
In skin wounds, macrophages play a central role in forming new blood vessels and re-epithelialization, ensuring the wound closes efficiently. In bone, specialized macrophages called “osteomacs” are critical supporters of osteoblast activity and bone matrix formation during regeneration. A study by Alexander et al. demonstrated that depleting osteomacs in a mouse tibial injury model severely hindered bone healing.
Cardiac repair highlights the importance of macrophage origin. In experimental models, resident cardiac macrophages in younger animals can support angiogenesis and repair with relatively controlled inflammation, whereas distinct recruited inflammatory monocyte–derived macrophages in adults are more often linked to fibrotic healing. In adult mice, however, the same injury attracts CCR2+ inflammatory monocytes, which tend to cause fibrosis instead of functional repair. In the liver, macrophages wear two hats: they contribute to scarring during injury through TGF-β signaling but later switch roles, producing matrix metalloproteinases that break down fibrotic collagen and help restore more normal liver architecture.
When macrophage signaling goes awry, though, the repair process can shift toward harmful fibrosis.
When Macrophage Activity Leads to Fibrosis
Macrophages are powerful agents of repair, but their activity needs to be carefully timed and balanced. If they fail to transition between states, the result can be pathological fibrosis, where excessive collagen buildup disrupts organ function.
Pathological fibrosis is frequently associated with prolonged profibrotic signaling, including TGF-β and type 2 cytokines such as IL‑13, from alternatively activated macrophages, which can drive excessive collagen deposition. Without a shift to the resolution phase (M2c macrophages), the ECM continues to accumulate without proper remodeling.This macrophage-driven profibrotic signaling is one important contributor to fibrosis in organs like the lungs, liver, and heart, alongside other cellular and molecular drivers.
"The timing and duration of M1 and M2 macrophage responses are critical for successful tissue repair... uncontrolled, prolonged, or excessive inflammatory activation is truly harmful." - Li Wang, Shaanxi University of Chinese Medicine
Interestingly, the ECM itself can influence macrophage behavior. Research from the University of Maryland, led by Associate Professor Erika Moore, revealed that the concentration of YIGSR - a peptide from the ECM protein laminin - affects macrophage activity. In that work, specific extracellular matrix–derived signals were shown to shift macrophage behavior toward either more repair-associated or more inflammatory phenotypes, highlighting how matrix composition can regulate macrophage activity. This feedback loop explains why heavily scarred, stiff tissue tends to stay inflamed instead of healing.
"By figuring out how they respond to signals from the extracellular matrix, we can start to develop treatments that help manage inflammation and support tissue repair in a more precise way." - Erika Moore, BIOE Associate Professor, University of Maryland
Key Takeaways and Next Steps
Linking Research Findings to Anatomy Education
Macrophages play a central role in tissue repair, handling everything from clearing debris to guiding the formation of blood vessels and connective tissue. Their ability to shift between activation states underlies processes that produce visible features in tissue, such as granulation tissue and collagenous scars seen in specimens. These microscopic cellular actions create the macroscopic features that are essential for understanding how tissues heal.
"Macrophages are highly plastic cells that continuously adapt to their environment and acquire phase-specific activation phenotypes." - Sebastian Willenborg et al., Department of Dermatology, University of Cologne
For anatomy educators, cadaveric specimens provide a unique opportunity to bridge the gap between cellular immunology and physical anatomical structures. For instance, observing a scar or granulation tissue during dissection offers a hands-on way to grasp the outcomes of macrophage activity. This connection enriches anatomical education while also inspiring new clinical approaches.
Clinical Uses and Future Research Directions
Timing is everything when it comes to macrophage-driven therapies. Suppressing inflammation too early can hinder the repair process, making it crucial to align treatments with the natural transitions of macrophage activity. Two promising areas of research stand out:
- Metabolic Modulation: Adjusting macrophage metabolism, such as shifting from glycolysis to oxidative phosphorylation, is being explored as a way to develop more targeted treatments for chronic wounds and impaired healing.
- Precision Targeting: Focusing on the CCR2-CCL2 recruitment pathway is being investigated as a strategy to limit pathological fibrosis in organs like the heart and liver while aiming to avoid broad immune suppression.
In a groundbreaking development, CARISMA Therapeutics launched a Phase I trial in 2020 for CT-0508, a Chimeric Antigen Receptor Macrophage (CAR-M) therapy aimed at HER2-overexpressing tumors. These advancements highlight the dual importance of macrophage research for both education and therapeutic innovation.
"Recognizing this mechanoregulation broadens therapeutic avenues for precisely modulating macrophage behavior in regenerative medicine." - Li Wang et al., Shaanxi University of Chinese Medicine
Resources for Further Study
To bring these insights into practice, educational tools are essential. The Institute of Human Anatomy offers a wealth of cadaver-based learning resources. Their interactive courses, detailed videos, and study guides showcase tissue-level changes, from the formation of an initial hemostatic plug to the development of dense collagenous scars. These materials are a valuable asset for students, educators, and healthcare professionals looking to connect cellular biology with gross anatomy in a meaningful way.
How Inflammation Really Works
FAQs
What makes macrophages switch from inflammation to repair?
Macrophages transition from an inflammatory role to one focused on repair as they respond to environmental signals during the healing process. Key influences include exposure to Th2 cytokines like IL-4 and IL-13, the clearance of apoptotic cells, and the detection of IL-10. These signals guide macrophages to resolve inflammation, shift to an anti-inflammatory state, and support tissue repair.
Why do some injuries heal with scars while others regenerate?
When it comes to healing, the outcome - whether it's regeneration or scarring - largely hinges on how the inflammatory response and macrophages are managed. Macrophages in balance play a key role in promoting tissue regeneration. On the flip side, when macrophages are out of sync, they can drive the overproduction of collagen, resulting in scarring. Key factors influencing this process include specific macrophage subsets and their regulation by factors such as macrophage colony-stimulating factor pathways and the timely shift from inflammation to repair. These elements are crucial for restoring function and avoiding fibrosis.
How does failed efferocytosis contribute to chronic wounds?
Failed efferocytosis disrupts the clearance of apoptotic cells, causing them to build up and undergo secondary necrosis. This process releases toxic substances and damage-associated molecular patterns (DAMPs), which fuel ongoing inflammation. Without resolving this inflammation or triggering anti-inflammatory responses, tissue repair stalls, resulting in a chronic, non-healing wound environment.

