
ACL Rehab Protocols: Evidence-Based Practices
Jun 02, 2026
Recovering from an ACL injury is no longer about following fixed timelines. Modern rehabilitation focuses on meeting specific milestones to safely restore strength, mobility, and confidence. This shift has been shown to reduce reinjury rates by up to 47% and improve return-to-sport outcomes.
Key Takeaways:
- Milestone-Based Recovery: Progression depends on achieving specific benchmarks, not arbitrary timelines.
- Prehabilitation Benefits: Structured pre-surgery programs improve recovery speed and return-to-sport rates.
- Objective Criteria: High strength and hop-test limb symmetry (commonly ≥90%) and adequate psychological readiness (for example ACL-RSI scores ≥70) are associated with better return-to-sport outcomes and may help reduce reinjury risk.
- Rehabilitation Phases: Early focus on swelling, full knee extension, and quadriceps activation transitions into strength, neuromuscular control, and advanced agility training.
- Return-to-Sport Testing: Athletes are often advised to meet strict criteria such as ≥90% limb symmetry on strength and hop tests, with assessment of hamstring and quadriceps strength, before clearance.
This approach prioritizes measurable progress, ensuring athletes return stronger and safer, while minimizing the risk of setbacks.
Shocking Look Inside a Torn ACL (Cadaver Dissection Revealed)
Preoperative Rehabilitation Phase
The period between injury and surgery plays a crucial role in recovery. Preoperative rehabilitation, often called "prehabilitation", aims to restore knee function before reconstruction. Research shows that patients who participate in structured prehab programs are more likely to return to their sport than those receiving standard care in several studies. Prehab can also speed up recovery, with some studies reporting that patients in prehabilitation programs return to sport several weeks earlier than those without prehab.
"The key to optimising ACL rehabilitation outcomes is to shift the focus of interventions to the preoperative phase, rather than concentrating solely on postoperative interventions." - van Melick
This underscores how targeted preoperative work can set the stage for better outcomes after surgery.
Preoperative Rehab Goals
The main goals of prehab include restoring full knee extension, reducing swelling for a "quiet knee", and building quadriceps strength. Achieving full extension is critical to minimizing the risk of arthrofibrosis after surgery, while strong quadriceps are vital for proper knee function during recovery. Between April 2023 and June 2024, a study at the Sana Medical Centre in Cologne tracked 114 participants. Those in a guided prehab program, attending two 60-minute supervised sessions weekly, improved their KOOS scores from 46.04 to 58.52 before surgery.
Exercises and Interventions
Prehab typically involves mobility exercises, strength training, and neuromuscular drills. For improving range of motion, exercises like supine knee extensions (using a towel roll under the heel) and heel slides are key. Passive knee extensions exercises should be performed regularly, within tolerance, to help ensure full straightening, following individualized guidance from the rehabilitation team. Strength training focuses on quadriceps sets, straight leg raises, and closed-chain exercises like double-leg quarter squats. Progressive loading is recommended: perform 3–4 sets of 6–8 reps and increase the weight when two additional reps can be completed.
In August 2025, a study at the Prince of Wales Hospital in Hong Kong explored the use of Whole-body Vibration (WBV) during prehab. Participants in the experimental group completed six 60-second squat sessions at 30 Hz, twice weekly for five weeks. Four months post-surgery, this group achieved significantly higher IKDC scores, with a mean difference of 5.60 compared to the control group. Neuromuscular training, such as perturbation drills on rocker boards and single-leg balance exercises, also prepares the knee for the challenges of early recovery. Effective programs typically last 4–6 weeks, with 2–4 sessions per week, helping ensure a smoother transition after surgery.
Postoperative Acute Phase
The first few weeks after ACL reconstruction surgery are critical for setting the stage for long-term recovery. Understanding the underlying human anatomy is essential for visualizing how these structures heal. As highlighted in a review from Sports Medicine:
"Early-stage rehabilitation is the vital foundation on which successful rehabilitation post-ACLR can occur. Without high-quality early-stage... rehabilitation, patients often do not overcome major aspects of dysfunction."
Meeting clinical discharge criteria was associated with an approximately 80–85% lower relative risk of reinjury in one cohort study. However, studies suggest that only a proportion of patients return to competitive sports, and in some cohorts of professional male soccer players, roughly two-thirds remain active at the top level three years after an ACL rupture. Below, we’ll outline the key interventions and milestones that define this acute phase of recovery.
Primary Goals
During the acute phase, rehabilitation focuses on four main objectives, each playing a critical role in recovery:
- Reducing swelling: Swelling can lead to arthrogenic muscle inhibition (AMI), which hinders proper muscle activation.
- Restoring full knee extension: A lack of full extension is linked to osteoarthritis and ongoing anterior knee pain.
- Activating the quadriceps: Overcoming AMI is essential to prevent muscle atrophy and rebuild strength.
- Improving movement quality: Proper movement patterns help normalize gait and support daily activities.
Early progress in knee extension and quadriceps strength is a strong predictor of long-term recovery. Failing to address these areas can lead to issues like knee instability, abnormal walking patterns, and even cartilage damage.
Treatment Interventions
Modern rehabilitation strategies increasingly adopt the POLICE model (Protection, Optimal Loading, Ice, Compression, Elevation), which updates the older PRICE approach by emphasizing optimal loading. This shift emphasizes the importance of controlled, early loading to support better outcomes.
Cryotherapy, paired with compression, is still vital for managing joint swelling. Studies indicate that cryotherapy can help reduce arthrogenic muscle inhibition (AMI), and there is limited evidence that adding electrical stimulation techniques may further support quadriceps activation after knee effusion. For patients struggling to activate their quadriceps voluntarily, neuromuscular electrical stimulation (NMES) is particularly effective, as it bypasses AMI and promotes muscle contraction.
Once swelling is under control and the quadriceps are activated, range of motion exercises become the next priority. Passive knee extensions are key to achieving full extension, with a pain level of 2–3/10 considered acceptable as long as the discomfort is short-lived. Evidence also supports incorporating open-kinetic chain (OKC) exercises, such as seated knee extensions, alongside closed-kinetic chain (CKC) movements like quarter squats. Early active extension not only prevents quadriceps atrophy but is also safe when done correctly .
Progression Milestones
Recovery during this phase should be guided by specific criteria to ensure a safe and effective transition to later stages. Important milestones include:
- Achieving full passive knee extension (0°)
- Minimal or no joint swelling, as measured by the Stroke test
- Performing a straight leg raise without any quadriceps lag
These benchmarks act as checkpoints, confirming the knee’s readiness to handle the greater demands of the next rehabilitation phase. Advancing too quickly - especially returning to sports before nine months - can increase the risk of reinjury by seven times.
Intermediate Phase: Strength and Neuromuscular Control
Once the milestones from the acute phase are achieved, the focus shifts toward restoring strength and reestablishing the brain-muscle connection. This phase builds on the early progress made during the acute phase, with the goal of preparing the body for the physical demands of activities like running, jumping, and cutting. Research highlights that key factors - such as isolated quadriceps strength - are often not fully recovered before athletes return to their sport.
Neuromuscular Training Methods
Neuromuscular training during this phase involves exercises that challenge both the body and mind. For example, neurocognitive drills like catching a ball while balancing or performing color-recognition tasks during single-leg exercises help rebuild neuromuscular connectivity. Instead of emphasizing internal cues, such as focusing on knee alignment, clinicians now use external feedback tools. A laser light system during step-down exercises, for instance, provides visual guidance to ensure proper lower limb alignment. Similarly, reactive agility drills using tools like Blaze Pods simulate the unpredictable nature of sports, training the nervous system to respond quickly while maintaining proper mechanics. These methods create a strong foundation for rebuilding strength in the next phase.
Strength Progression
Rebuilding muscle strength requires a structured approach targeting the quadriceps, hamstrings, calf muscles, and hip complex. Blood flow restriction (BFR) training is increasingly used alongside traditional resistance exercises and, in some studies, has improved strength and function with relatively low mechanical loads, which may help limit stress on healing joints. Strength progression protocols, such as DAPRE or the +2 principle, adjust exercise loads based on performance feedback.
Interestingly, research shows that even when double-leg squats appear symmetrical, individuals often reduce knee loading by about 20% on the injured side, compensating with the hip or the uninjured leg. This subtle imbalance, known as a "controlled knee moment", can go unnoticed without tools like force plates or detailed video analysis. Before advancing to running, basic plyometric exercises like double- and single-leg pogo hops are effective for assessing load acceptance. Objective benchmarks help determine readiness for the more demanding advanced phase.
Advancement Criteria
Progression to the advanced phase depends on meeting specific benchmarks rather than just following a timeline. Athletes should achieve 70–80% limb symmetry in quadriceps strength during this stage, with many protocols using 90% or higher as one of several criteria before returning to their sport. Functional performance tests, are often targeted to show less than 10% asymmetry, and the knee should exhibit minimal swelling (effusion less than 1 cm compared to the uninjured side).
| Criteria Category | Measurement Method | Target for Advancement |
|---|---|---|
| Quadriceps Strength | Handheld Dynamometer | 70–80% Limb Symmetry Index (LSI) |
| Functional Performance | Single-Leg Hop Tests | <10% asymmetry (≥90% symmetry) |
| Joint Health | Sweep Test for Effusion | Effusion <1 cm compared to the uninvolved side |
| Pain Level | Visual Analog Scale | <3/10 during and after exercise |
"Time is not an indicator of function. Recent studies show that while ligamentization takes time, the physical and neuromuscular readiness of a patient varies greatly from one individual to another".
Advancement should always align with objective functional measures, as returning too soon significantly increases the risk of reinjury.
Advanced Phase: Power, Agility, and Return to Sport
The final stage of ACL rehabilitation is all about getting athletes back to peak performance. This phase emphasizes explosive movements, quick decision-making, and rebuilding the confidence needed to handle the unpredictable nature of sports. Pre-planned agility drills, while helpful, don’t fully replicate the mental and physical demands of competition. That’s where reactive agility training steps in. By introducing external cues like flashing lights or timing gates, athletes are forced to make split-second decisions, mimicking real-game scenarios. Systems like Smartspeed bring these challenges to life, creating a foundation for the next steps in power and agility training.
Power and Agility Training
To build explosive power, the focus shifts from just increasing maximum strength to improving the Rate of Force Development (RFD) - essentially, how quickly an athlete can produce force. This is crucial for actions like jumping, sprinting, and cutting. Tools like the Isometric Mid-Thigh Pull (IMTP) on force plates provide a comprehensive way to measure explosive strength and posterior chain function, offering more relevant insights than isolated tests.
Advanced plyometric exercises, such as depth jumps and reactive hops, challenge the neuromuscular system to produce force quickly while maintaining proper form. Training under fatigue is also key - it can reveal movement flaws and highlight areas at risk for re-injury. For example, sport-specific drills like cutting maneuvers after a conditioning circuit simulate game-day stress and prepare the body for competition.
Athletes often struggle with cutting in one direction, showing deficits in speed and confidence. Addressing this directional asymmetry through targeted testing and training is essential. Once explosive strength is developed, objective testing ensures athletes are ready to compete.
Return-to-Sport Testing
Getting the green light for competition requires a thorough testing process that evaluates strength, power, agility, and mental readiness. A Limb Symmetry Index (LSI) of 90% or higher is commonly used as a benchmark for strength and hop tests, although it may not fully capture true recovery. However, LSI can be misleading since the uninjured limb often weakens during rehab. To help assess knee muscle balance, many protocols aim for a hamstring-to-quadriceps (H/Q) strength ratio around 80% to 85%, although exact thresholds vary between programs. Some studies suggest that unfavorable hamstring-to-quadriceps strength profiles are associated with a higher risk of a second ACL injury, but the exact risk increase and cut-off values are still being investigated.
Psychological readiness is equally important. The ACL-RSI scale measures confidence, with a target score of 75 to 90 depending on the protocol. A 15-point improvement on this scale is considered clinically meaningful. Interestingly, research shows a moderate negative correlation between Reactive Agility Test (RAT) times and ACL-RSI scores - athletes who are faster and more agile tend to feel more confident.
Emerging research suggests that protocols combining strength symmetry, favorable H/Q ratios, hop performance, and higher ACL-RSI scores may lower re-injury risk compared with relying on time since surgery alone, although the exact percentage risk reduction varies between studies. Systematic reviews suggest that a majority of athletes, often around 60 to 85 percent depending on level and sport, can return to their pre-injury level of play after ACL reconstruction, although outcomes vary widely. These findings reinforce the importance of milestone-based progress in rehab.
Recovery Timelines
The advanced phase typically spans 6 to 12 months post-surgery, but recovery isn’t just about hitting a certain date. While graft remodeling is thought to take many months, often extending toward a year, returning too soon increases the risk of re-injury and can set recovery back. Studies estimate around 15–20% re-injury rate within 24 months of ACL reconstruction, with nearly half of these occurring in the first year. Factors like graft type, age, and meniscus damage play a significant role in recovery timelines.
Systematic reviews indicate that more than 80% of elite and professional athletes return to sport after ACL reconstruction, with roughly 80–90% of those who return achieving their preinjury level. In contrast, among recreational athletes, around 60% typically regain their pre-injury level of sport. Regardless of the athlete’s level, progression to advanced training should be avoided if the knee shows swelling or lacks full range of motion. Even after clearance, ongoing secondary injury prevention during competition is essential to reduce long-term risks. Ultimately, functional recovery - not arbitrary deadlines - should dictate the pace of this phase.
Comparing ACL Rehab Protocols
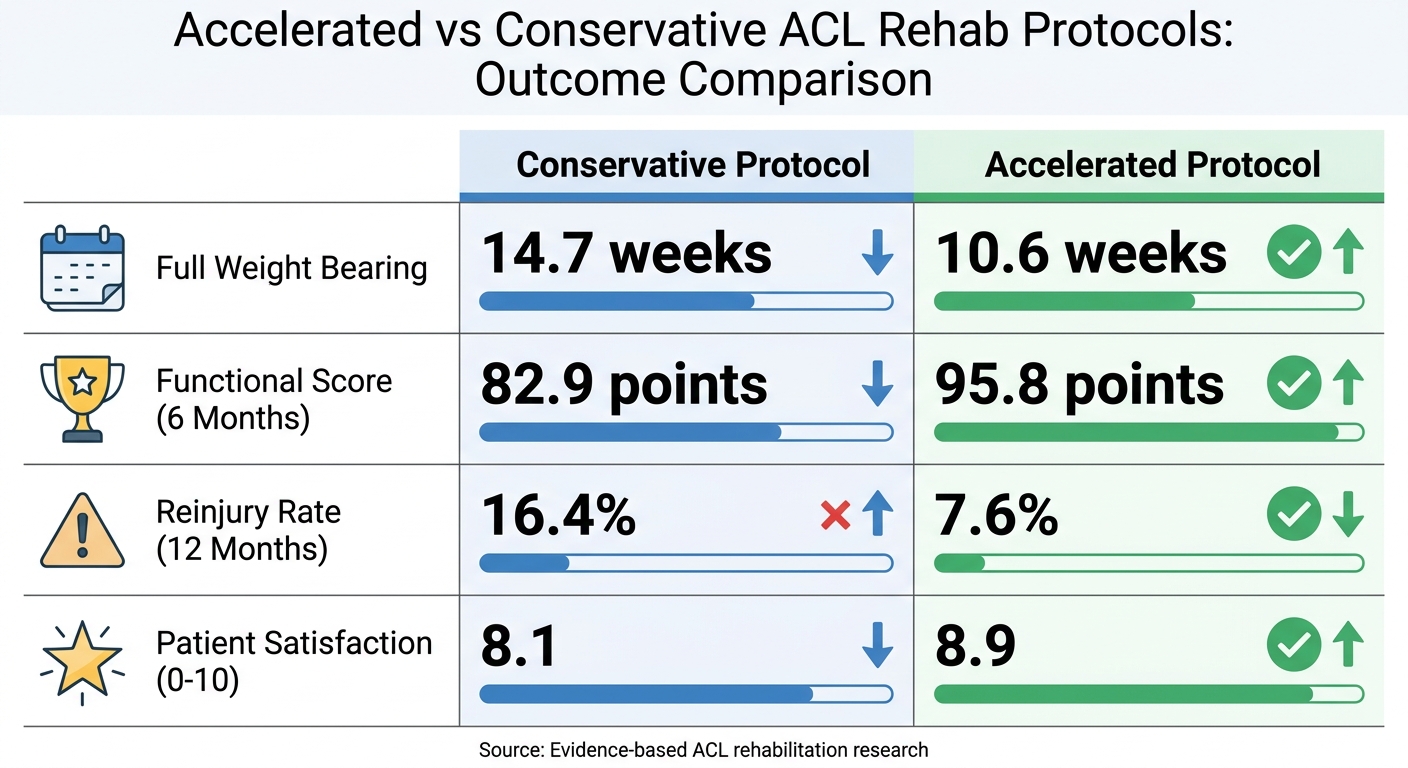
Accelerated vs Conservative ACL Rehab Protocol Outcomes Comparison
When it comes to ACL rehabilitation, not all protocols are created equally. Over the years, research has revealed key differences in recovery outcomes between approaches. While conservative protocols take a slower, more cautious route to protect the healing graft, modern studies have begun to challenge this perspective. The debate between accelerated and conservative strategies has brought attention to how recovery can take different paths.
Accelerated vs. Conservative Protocols
Accelerated protocols, such as those outlined in the Aspetar Guidelines, focus on a faster, milestone-based recovery approach rather than adhering to strict timelines. These protocols aim to achieve specific goals like strength and movement quality before progressing. For instance, some studies report that accelerated rehabilitation protocols achieve full weight-bearing earlier than more conservative methods, although the exact timelines vary between protocols. Some randomized trials have found that accelerated rehabilitation protocols can lead to higher short‑term functional scores and similar patient satisfaction compared with more conservative protocols, although results and reinjury rates differ between studies.
| Variable | Conservative Protocol | Accelerated Protocol |
|---|---|---|
| Full Weight Bearing | 14.7 weeks | 10.6 weeks |
| Functional Score (6 Months) | 82.9 points | 95.8 points |
| Reinjury Rate (12 Months) | 16.4% | 7.6% |
| Patient Satisfaction (0-10) | 8.1 | 8.9 |
The core difference lies in philosophy. Conservative protocols prioritize a slower pace to safeguard the graft, while accelerated approaches focus on restoring function using objective criteria like strength and range of motion. Importantly, many studies report that accelerated protocols can improve function without clearly worse patient-reported outcomes, although some evidence suggests they may be associated with greater knee laxity and tunnel widening, so they should be applied with caution.
New Techniques and Future Directions
Looking forward, the trend in ACL rehabilitation is moving toward personalized plans tailored to each individual's injury and activity needs. With the success of accelerated strategies, new tools and surgical advances are helping refine the process even further. Instead of sticking to rigid timelines, clinicians now consider factors like graft type, age, meniscus damage, and the athlete’s specific sport.
Technology is also reshaping the field. Tools like smartphone apps, handheld dynamometers, and standardized clearance checklists make it easier to track progress with objective measures. Additionally, innovative techniques like Blood Flow Restriction (BFR) training and Neuromuscular Electrical Stimulation (NMES) are proving useful for patients dealing with early muscle atrophy or those who can’t tolerate heavy joint loads.
On the surgical side, emerging methods such as BEAR (Bridge-Enhanced ACL Repair), DIS (Dynamic Intraligamentary Stabilization), and IBLA (Internal Brace Ligament Augmentation) offer alternatives to traditional reconstruction, particularly for acute proximal tears. However, these repair techniques come with challenges, including concerns about higher failure or reoperation rates in some reports and issues such as hardware irritation requiring removal, and long‑term comparative data with autograft reconstruction are still limited. For now, these methods are most effective when surgery occurs within 21 days of injury and involves a proximal avulsion.
The shift toward milestone-based progression continues to gain traction. Moving beyond the traditional nine-month timeline for return-to-play, multi-criteria protocols are proving to be more effective. These approaches often use benchmarks such as high hamstrings-to-quadriceps strength ratios, hop and strength limb symmetry indexes near or above 90%, and sufficient psychological readiness scores (for example ACL-RSI scores around 70–75) to guide readiness. By focusing on functional recovery rather than time, these strategies significantly reduce reinjury risks and align with the latest research.
Conclusion
Moving away from fixed timelines to evidence-based, criterion-driven protocols marks a major shift in how ACL rehabilitation is managed. Research shows that delaying return to high-risk sports to at least 9 months after surgery and using multi-test, criterion-based clearance are associated with substantially lower reinjury risk compared with earlier, time-based return. Athletes following structured, criterion-based protocols in some cohorts have demonstrated high rates of return to their pre-injury level of sport. This distinction highlights the balance between safely returning to competition and minimizing the need for reoperation.
The importance of objective testing in recovery cannot be overstated. Achieving specific benchmarks in strength, functional performance, and psychological readiness is key. For instance, many RTS batteries use benchmarks such as a limb symmetry index of around 90% in quadriceps strength and hop tests and ACL-RSI scores around 70–75; hamstring-to-quadriceps strength ratios are also assessed, although exact cut-off values are not firmly established. Meeting stringent objective benchmarks on strength, functional tests, and psychological readiness has been associated with markedly lower second ACL injury rates within the first 1–2 years after return to sport.
Rehabilitation, however, doesn’t stop at clearance for sport. Long-term joint health depends on continuous care, including secondary prevention programs aimed at reducing risks like osteoarthritis and contralateral injuries. A great example is the University of Delaware's ACL-SPORTS program. Between 2013 and 2017, their use of regular quadriceps strength assessments and milestone-based progressions was accompanied by a remarkably low 2-year reinjury rate of 2.5% in one trial. This success illustrates how integrating milestone-driven strategies creates a comprehensive recovery plan.
The takeaway is clear: rehabilitation is not about waiting for time to pass. It’s about achieving measurable milestones, addressing both physical and mental readiness, and following proven, evidence-based practices. Whether you’re a clinician or an athlete, these protocols provide a clear path to recovering safely and returning to the activities you love.
FAQs
How do I know if I’m ready to start running after ACL surgery?
You can start running after ACL surgery once you hit key milestones like having enough quadriceps strength, proper movement mechanics, and being free of pain or swelling. A healthcare professional will check your strength, stability, and how well you move to make sure you're ready. Using a criterion-based approach helps lower the chance of reinjury. Always work with your physical therapist or sports medicine specialist to get a tailored assessment before moving forward.
What tests determine if I can return to sport?
Tests for returning to sport after ACL reconstruction often involve a mix of functional assessments and readiness evaluations. Key benchmarks include achieving a limb symmetry index (LSI) near or above 90%, scoring 75% or higher on the ACL-RSI scale, and completing milestone-based tests like hop tests and strength assessments. These tools are designed to reduce the risk of re-injury and promote a safe return to physical activity.
Why can limb symmetry scores be misleading?
Limb symmetry scores might give the impression that an athlete is ready to return to sports, but they can be deceptive. These scores often overlook critical factors like functional deficits or the risk of re-injury. Studies highlight that focusing solely on symmetry indices can fail to capture the full picture of recovery. This means hidden issues affecting performance and long-term health might go unnoticed, potentially jeopardizing the athlete's safety.

