
Common Sports Injuries: Ligament Sprains Graded
Jun 21, 2026
Ligament sprains are one of the most frequent sports injuries, often underestimated but requiring proper care to avoid long-term issues like joint instability. Here's what you need to know:
- What is a ligament sprain? It occurs when ligaments, the tough tissues connecting bones, are overstretched or torn.
- Commonly sprained joints: Ankles (most frequent), knees, and wrists.
- Sprain severity grades:
- Grade 1: Mild stretching, stable joint, recovery in days to 2 weeks.
- Grade 2: Partial tear, some instability, recovery in weeks.
- Grade 3: Complete tear, unstable joint, recovery in 6–12 weeks or more, sometimes requiring surgery.
- Key causes: Movements like ankle inversion, knee valgus stress, or rapid pivoting during sports like soccer, basketball, and football.
- Treatment: Initial care follows the POLICE principle (Protection, Optimal Loading, Ice, Compression, Elevation). Rehabilitation focuses on reducing inflammation, restoring motion, and strengthening the joint.
- Prevention tips: Strength training, balance exercises, proper equipment (e.g., ankle braces), and safe techniques reduce the risk of sprains.
Understanding the severity and proper management of ligament sprains is critical for effective recovery and preventing future injuries. Always seek professional evaluation for severe symptoms like joint instability or inability to bear weight.
Ligament Anatomy and How Injuries Happen
Ligament Structure and Function
Ligaments are tough, connective tissue bands that connect bones, playing a key role in stabilizing joints. They’re made up mostly of tightly packed Type I collagen fibers, which give them their strength and structure. These fibers have a unique wavy pattern, called a crimp, that allows ligaments to stretch slightly under light loads before becoming taut, resisting further movement.
What’s fascinating is that ligaments are viscoelastic, meaning their response depends on how quickly or for how long a force is applied. This property helps them absorb sudden stresses while maintaining joint stability. Ligaments are also packed with nerve endings that provide proprioceptive feedback, helping the brain sense joint position. When ligaments are injured, this feedback can be disrupted, affecting coordination and movement. Understanding this structure helps explain why quick, forceful sports movements often lead to ligament injuries.
How Sports Movements Cause Ligament Sprains
Ligament sprains happen when a joint is pushed beyond its normal range of motion in a very short time. Two common ways this occurs are through ankle inversion and knee valgus stress.
- Ankle Inversion: This happens when the foot rolls inward, often leading to lateral ankle sprains. The anterior talofibular ligament (ATFL) is most commonly affected. Each year, more than 2 million acute ankle sprains are treated in the United States.
- Knee Valgus Stress: This involves an inward force on the knee, often during a tackle or collision. It typically strains the medial collateral ligament (MCL) and sometimes the anterior cruciate ligament (ACL). Movements like rapid pivoting or cutting, which force the knee to change direction suddenly, are also major culprits. Interestingly, over half of ACL injuries in team ball sports are non-contact, with an even higher proportion in female athletes. Females are about 2 to 5 times more likely than males to experience an ACL rupture in similar sports environments.
Tearing the Meniscus & MCL
Here’s a quick breakdown of common injury mechanisms and the ligaments they affect:
| Movement | Joint | Primary Ligament(s) at Risk | Common Sports |
|---|---|---|---|
| Inversion | Ankle | ATFL, CFL | Basketball, soccer, trail running |
| Valgus stress | Knee | MCL, ACL | Football, soccer |
| Rapid pivoting or cutting | Knee | ACL | Basketball, football, soccer |
| Hyperextension | Knee | ACL, PCL | Gymnastics, sudden stops |
| Eversion | Ankle | Deltoid ligament, syndesmosis | Collision sports |
These patterns highlight how essential it is to understand ligament anatomy for assessing and managing injuries effectively.
How Anatomy Knowledge Supports Injury Assessment
A solid grasp of ligament anatomy makes injury evaluation much more precise. For example, the ACL as a whole is the primary ligament resisting forward tibial translation, with its bundles playing major roles in controlling this motion. This insight helps clinicians perform stress tests, like the Lachman test, with greater accuracy. The Lachman test, for instance, shows pooled sensitivities around 75–80% and high specificity for detecting ACL tears, making it one of the most useful clinical tests.
Cadaver-based learning offers an unparalleled way to observe how ligaments behave under stress. Programs like those at the Institute of Human Anatomy use real cadavers to help students and healthcare professionals see firsthand how specific forces can lead to ligament damage. This hands-on approach deepens understanding and improves both diagnosis and treatment.
"Ligaments are best suited to transfer load from bone to bone along the longitudinal direction of the ligament." - Savio L.-Y. Woo, PhD, D.Sc., University of Pittsburgh
This principle is crucial in clinical assessments. When a force is applied at an angle outside a ligament’s primary axis - like during an awkward landing or sudden pivot - the risk of injury increases significantly.
Shocking Look Inside a Torn ACL (Cadaver Dissection Revealed)
Ligament Sprain Grades: Severity and Symptoms
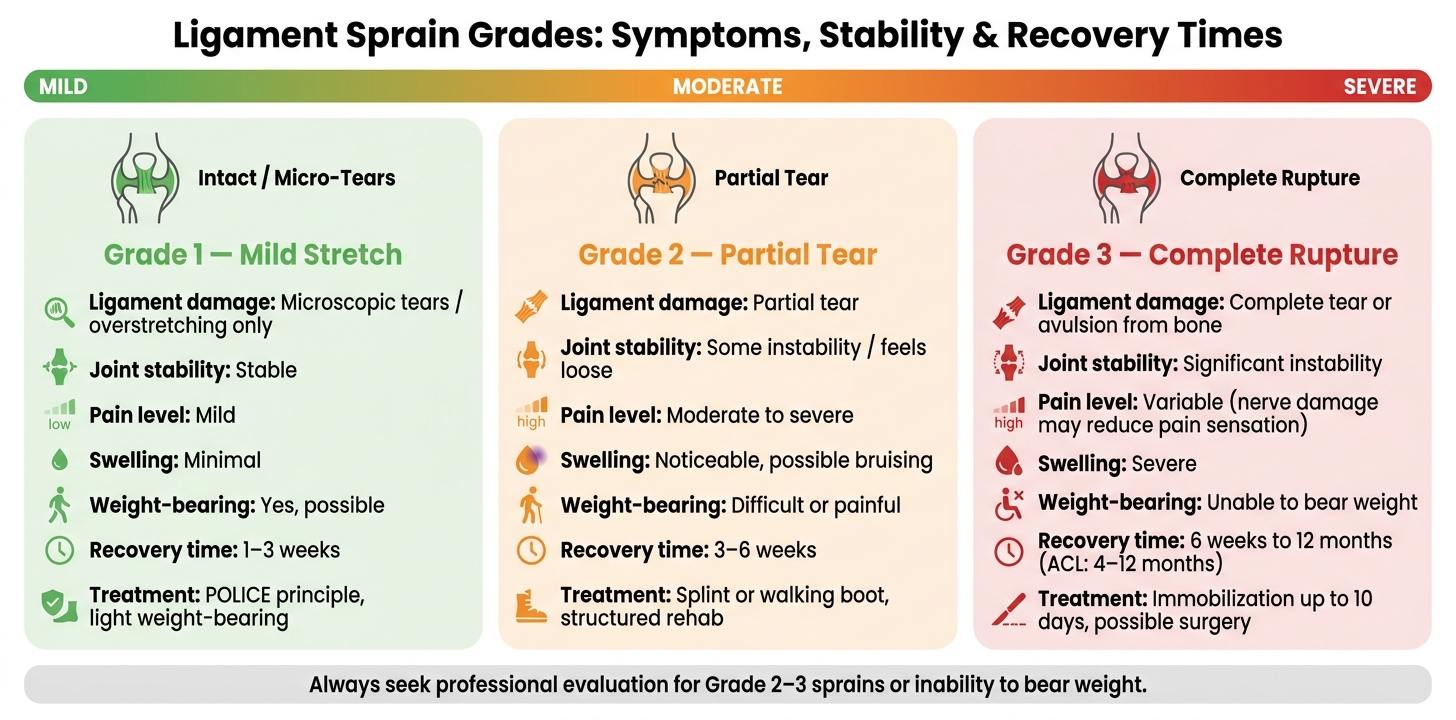
Ligament Sprain Grades: Symptoms, Stability & Recovery Times
Understanding the severity of ligament sprains is crucial for planning treatment and recovery. These injuries are divided into three grades based on the extent of ligament damage and how much the joint's stability is affected. Each grade comes with its own set of symptoms and recovery timelines.
Grade 1 Sprains: Mild Ligament Stretching
Grade 1 sprains involve a mild stretch or tiny tears in the ligament fibers, but the joint remains stable. Symptoms include mild pain and minimal swelling, and most people can still walk and bear weight. These injuries often happen during everyday athletic movements, like rolling an ankle on uneven ground or slipping slightly during a quick direction change. Recovery usually takes about 1 to 3 weeks.
Grade 2 Sprains: Partial Ligament Tears
In a Grade 2 sprain, the ligament is partially torn, which leads to some loss of joint stability. This type of injury typically causes moderate to severe pain, noticeable swelling, and sometimes bruising. Walking can be difficult or painful, and the joint may feel loose, signaling the ligament isn't fully supporting it. Common causes include awkward landings in basketball or sharp directional changes in soccer. Recovery generally takes 3 to 6 weeks, and rehabilitation is crucial to restore joint stability and avoid long-term issues.
Grade 3 Sprains: Complete Ligament Ruptures
A Grade 3 sprain means the ligament is completely torn, or in some cases, it may even detach from the bone (avulsion). This causes significant joint instability, and the individual is usually unable to put weight on the affected limb. Interestingly, pain might not be as intense because the nerve fibers in the ligament are often damaged.
"In severe cases, the sprained joint can become unstable and loose, bones can move out of alignment, and the joint may extend beyond its normal range of motion." - Harvard Health Publishing
These injuries often result from high-impact events, such as landing on another player’s foot, a hard fall while skiing, or a high-speed collision. Recovery can range from 6 weeks to several months, and for severe cases like an ACL rupture, it may take 4 to 12 months. Imaging techniques like X-rays can rule out fractures, while MRIs are used to assess the severity especially when serious injury is suspected or when symptoms do not improve with initial care. Surgery is sometimes required, depending on the joint, the athlete's activity level, and the degree of instability.
This grading system helps guide treatment plans and ensures rehabilitation is tailored to the injury's severity.
Managing and Rehabilitating Ligament Sprains
Immediate Care After a Sprain
When dealing with a sprain, the first priority is to protect the injured joint and manage swelling. The POLICE principle - Protection, Optimal Loading, Ice, Compression, Elevation - is widely promoted in sports medicine, although high-quality evidence for the overall protocol is limited. To reduce pain and swelling, short bouts of ice application (for example, around 15–20 minutes at a time) during the first 24–48 hours may help with pain and swelling. Pair this with compression, such as an elastic bandage, and elevate the limb above heart level to minimize fluid buildup (edema).
For a Grade 1 sprain, a short period of protection with light, early weight-bearing is usually enough. Grade 2 sprains might need additional support, like a splint or walking boot, while Grade 3 sprains may require a short period of immobilization before starting rehabilitation. If the injury involves bone tenderness or if walking four steps causes significant pain, it’s essential to get a medical evaluation. The Ottawa Ankle Rules can help determine if an X-ray is necessary. Once swelling is under control and pain decreases, structured rehabilitation becomes the next critical step.
Rehabilitation and Recovery Methods
After the initial care phase, a well-organized rehabilitation plan is key to a complete recovery. Rehabilitation typically follows three phases:
- Phase 1: Focuses on reducing inflammation and protecting the injured area.
- Phase 2: Aims to restore range of motion and rebuild strength with exercises like calf raises and ankle circles.
- Phase 3: Introduces neuromuscular and proprioceptive training, such as single-leg balance exercises and wobble board activities, to improve joint stability.
"Early functional rehabilitation, rather than prolonged immobilization, promotes optimal recovery." - StatPearls
Proprioceptive training is especially important because sprains can damage the nerve endings that help your body sense joint position. Without proper rehabilitation, proprioceptive and other sensorimotor deficits are associated with chronic instability, which occurs in roughly 20–40% of people after a lateral ankle sprain. One effective tool for rebuilding proprioceptive control is Short Foot Exercises (SFE). These exercises can be progressed from seated positions to single-leg stances over an 8–9 week period.
Return-to-Play Guidelines
One of the most common mistakes after a sprain is returning to sports too soon. Athletes with lateral ankle sprains are twice as likely to reinjure themselves within a year of the initial incident. Decisions about resuming play should be based on meeting specific functional milestones, not just the absence of pain at rest. The PAASS framework is a helpful guide, evaluating:
- Pain
- Ankle impairments
- Athlete perception
- Sensorimotor control
- Sport-functional performance
This means ensuring a full, pain-free range of motion, balanced strength between both sides, successful performance on balance tests (like the Star Excursion Balance Test), and the ability to complete sport-specific agility drills without feeling unstable. For added protection, using a semi-rigid brace or taping after returning to play is recommended for a period determined with a clinician, especially in the first months back.
"Surgery should be reserved for cases that do not respond to thorough and comprehensive exercise-based treatment." - British Journal of Sports Medicine
How to Reduce the Risk of Ligament Sprains
Preventing ligament sprains isn't just about treatment - it's about taking proactive steps to minimize future injuries.
Strength and Neuromuscular Training
Prevention programs that combine strength, balance, and movement training are highly effective. Research shows that programs with multiple components lower the risk of lower-extremity injuries more than single-focus ones (with pooled risk ratios around 0.67 compared with higher values for single-focus programs in some analyses). For example, targeting muscles like the tibialis anterior, tibialis posterior, and extensor hallucis longus through neuromuscular and strength exercises helps build ankle inversion strength. Core exercises include Nordic hamstring curls, lunges, heel-calf raises, and single-leg balance drills. Ideally, these exercises should be done 2–3 times a week, with each session lasting 20–24 minutes.
"Lower extremity muscle strength and balance exercises should be prioritised in lower extremity injury prevention programmes for team-sport athletes." - British Journal of Sports Medicine
Including balance-focused neuromuscular training in these programs has been shown to substantially reduce ACL injury risk, particularly in female athletes. Consistency is also key - studies indicate that higher adherence to prevention programs is associated with larger reductions in injury risk. Starting these programs during middle or high school, when movement habits are still forming, can have a long-lasting impact.
To further protect at-risk joints, strength training can be combined with external supports.
Protective Equipment and Safe Technique
Using proper equipment and techniques can make a big difference. Semi-rigid ankle braces are at least as effective as athletic tape and may be more practical during extended activity. While tape loses 40–50% of its support after just 15 minutes, braces maintain their effectiveness, are reusable, and are less likely to cause skin irritation. For athletes with a history of ankle sprains, the National Athletic Trainers' Association advises wearing these braces during both practices and games.
Landing techniques also matter. The anterior talofibular ligament (ATFL) is involved in the majority of lateral ankle sprains; landing and cutting techniques that avoid excessive plantarflexion and inversion are generally recommended to reduce strain on this ligament. Playing surfaces are another factor: some studies suggest that ankle sprain risk differs between artificial turf and natural grass in soccer, although the exact risk estimates vary. Proper footwear tailored to the playing surface is essential for maintaining traction and minimizing injury risk.
How Anatomical Education Supports Injury Prevention
Understanding joint anatomy can significantly enhance injury prevention strategies. Athletes and coaches who know that the ankle is most vulnerable in a plantar-flexed and inverted position - its least stable state - can train to avoid or control that position under load. Knowing that the ATFL absorbs inversion forces and that female athletes have, on average, a higher risk of ACL injuries than males, influenced by anatomical, hormonal, and biomechanical factors, helps translate these risks into actionable training goals.
Organizations like the Institute of Human Anatomy provide cadaver-based anatomy education, offering a three-dimensional view of ligament structures, joint capsules, and surrounding muscles. This kind of detailed understanding helps athletes, trainers, and clinicians design better movement training, rehabilitation plans, and injury prevention strategies.
"Integrating biomechanical and molecular insights can optimize ankle sprain management." - Bone & Joint Research
Conclusion: Understanding Ligament Sprains from Diagnosis to Prevention
Grasping the entire process of managing ligament sprains - from identifying the injury to preventing recurrence - is key to effective care.
Ligament sprains can range from mild to severe. For example, Grade I sprains often recover over a period of days to a few weeks, while Grade III ruptures, like ACL tears, often demand a recovery period of 6 to 12 months. Accurate grading plays a critical role in guiding treatment and reducing the risk of long-term issues.
Getting the diagnosis right is essential. ACL injuries are common in athletes, and many involve complete ligament ruptures that require prolonged rehabilitation, but precise annual counts and the exact proportion of complete ruptures vary between studies. Mismanaging ankle sprains, on the other hand, can lead to ongoing instability. The good news? Most Grade I and II sprains heal completely with proper conservative care. Timing also matters. Stress tests performed 4 to 5 days post-injury are far more reliable than immediate assessments, boasting an 84% sensitivity and 96% specificity for identifying ligament ruptures. Performing these tests too soon can lead to underestimating the injury due to pain and spasms masking ligament laxity, which may result in inadequate treatment.
"Early functional rehabilitation is preferred over prolonged immobilization, as it promotes ligamentous healing and restores joint stability." - StatPearls
A solid understanding of ligament anatomy is vital at every stage of injury management. This includes knowing which ligaments are most vulnerable in specific movements, like inversion injuries, and tailoring rehabilitation programs to address proprioceptive deficits caused by severe tears. Resources like the Institute of Human Anatomy provide valuable learning opportunities through cadaver-based education, offering athletes, coaches, and clinicians a three-dimensional understanding that aids in designing effective prevention and recovery strategies.
FAQs
How can I tell if a sprain is Grade 2 or Grade 3?
A Grade 2 sprain occurs when the ligament is partially torn. This typically results in noticeable swelling, bruising, tenderness, and discomfort when walking. On the other hand, a Grade 3 sprain is much more severe, involving a complete tear of the ligament. Symptoms include intense swelling, joint instability, and difficulty or inability to bear weight on the affected area.
Healthcare providers may perform stress tests, such as the anterior drawer test, to evaluate joint stability. Significant movement in the joint during these tests often points to a Grade 3 tear.
When should I get an X-ray or MRI for a sprain?
Most sprains are diagnosed by reviewing the patient's medical history and performing a physical exam. If there are signs of possible bone damage, or if specific criteria like the Ottawa ankle rules indicate it, an X-ray might be required to rule out fractures. While an MRI isn't typically needed right away, it can be useful for assessing severe injuries or persistent pain lasting more than six weeks, particularly to detect tears or less obvious problems.
What tests confirm it’s safe to return to play?
The PAASS framework is designed to determine an athlete's readiness to get back in the game by focusing on five key areas: pain levels, ankle impairments, athlete perception, sensorimotor control, and functional performance. To evaluate these, tests like the dorsiflexion lunge test, star excursion balance test, agility T-test, and vertical jump test are commonly used. Alongside these physical assessments, psychological readiness and sport-specific drills are also considered to confirm the athlete has the necessary stability and strength to return safely to their sport.

